EUROLINE
positive control serum: IgG, human, 100x concentrated
for DL 1111-1 G, DL 1111-2 G, DL 1111-4 G and DL 1111-7 G
IIFT
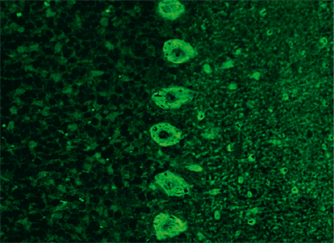
brain: grey and white matter,
Purkinje cell cytoplasm (Yo),
Hu and Ri antigen
CV2, Ma, amphiphysin
cerebellum
monkey
IIFT
Neurology Mosaic 1
Yo, Hu, Ri, CV2, Ma, amphiphysin
medullated nerves
non-medullated nerves
3 BIOCHIPs per field:
cerebellum
nerves
intestinal tissue
monkey
monkey
monkey
IIFT
Neurology Mosaic 1 EUROPattern
Yo, Hu, Ri, CV2, Ma, amphiphysin
medullated nerves
non-medullated nerves
3 BIOCHIPs per field:
cerebellum
nerves
intestinal tissue
monkey
monkey
monkey
IIFT
Neurology Mosaic14
cerebellum antigens
non-medullated nerves
2 BIOCHIPs per field:
cerebellum
intestinal tissue
monkey
monkey
IIFT
Neurology Mosaic14
cerebellum antigens
non-medullated nerves
2 BIOCHIPs per field:
cerebellum
non-medullated nerves
monkey
monkey
IIFT
Neurology Mosaic 14 EUROPattern
cerebellum antigens
medullated nerves
2 BIOCHIPs per field
cerebellum
intestinal tissue
monkey
monkey
IIFT
Yo, Hu, Ri, CV2, Ma, amphiphysin
medullated nerves
non-medullated nerves
cell nuclei (ANA)
cerebellum
nerves
intestinal tissue
HEp-2 cells
(4 BIOCHIPs per field)
monkey
monkey
monkey
human
IIFT
Neurology Mosaic 17
Yo, Hu, Ri, CV2, Ma, amphiphysin, NMO
cerebrum antigens, NMO
NMO, optic nerve antigens
aquaporin-4
5 BIOCHIPs per field
cerebellum
cerebrum
optic nerve
transfected cells
control transfection
monkey
monkey
monkey
EU 90
EU 90
EUROLINE
Neuronal Antigens Profile 2
(amphiphysin, CV2, PNMA2
(Ma-2/Ta), Ri, Yo, Hu separately)
EUROLINE
IIFT
Neurology Mosaic 2
Yo, Hu, Ri, CV2, Ma, amphiphysin
medullated nerves
2 BIOCHIPs per field:
cerebellum
nerves
monkey
monkey
EUROLINE
Neuronal Antigens Profile PLUS RST
(amphiphysin, CV2, PNMA2
(Ma-2/Ta), Ri, Yo, Hu,
recoverin, SOX1, titin separately)
EUROLINE
EUROLINE
positive control serum: IgG, human, 100x concentrated
for DL 1111-6 G
EUROLINE
Neuronal Antigens Profile
SOX1, titin
EUROLINE
EUROLINE
Paraneoplastic Neurologic Syndromes - 12 Ag
(amphiphysin, CV2, PNMA2 (Ma-2/Ta), Ri, Yo, Hu,
recoverin, SOX1, titin, Zic4, GAD65, Tr (DNER) separately)
EUROLINE
IIFT
Neurology Mosaic 8
Yo, Hu, Ri, CV2, Ma, amphiphysin
medullated nerves
non-medullated nerves
pancreas islets
4 BIOCHIPs per field
cerebellum
nerves
intestinal tissue
pancreas
monkey
monkey
monkey
monkey
IIFT
Neurology Mosaic 8 EUROPattern
Yo, Hu, Ri, CV2, Ma, amphiphysin
medullated nerves
non-medullated nerves
pancreas islets
4 BIOCHIPs per field:
cerebellum
nerves
intestinal tissue
pancreas
monkey
monkey
monkey
monkey
IIFT
antibodies against neuronal nuclei: Hu antigen
(Hu ab control)
Secondary reagents immunoblot (IgA)
Additional Reagents
EUROLINE (IgE)
Secondary reagents immunoblot (IgG)
Secondary reagents immunoblot (IgM)



















 New diagnostic criteria for PNS have recently been established (Graus et al., 2020). What is new is the subdivision into high-risk phenotypes (encephalomyelitis, limbic encephalitis, rapidly progressive cerebellar syndrome, opsoclonus-myoclonus syndrome, sensory neuronopathy, gastrointestinal pseudoobstruction (enteric neuropathy), Lambert-Eaton myasthenic syndrome) and intermediate-risk phenotypes for PNS (including encephalitis, anti-NMDA receptor encephalitis, brainstem encephalitis, Morvan syndrome, isolated myelopathy, stiff-person syndrome, polyradiculoneuropathy).
New diagnostic criteria for PNS have recently been established (Graus et al., 2020). What is new is the subdivision into high-risk phenotypes (encephalomyelitis, limbic encephalitis, rapidly progressive cerebellar syndrome, opsoclonus-myoclonus syndrome, sensory neuronopathy, gastrointestinal pseudoobstruction (enteric neuropathy), Lambert-Eaton myasthenic syndrome) and intermediate-risk phenotypes for PNS (including encephalitis, anti-NMDA receptor encephalitis, brainstem encephalitis, Morvan syndrome, isolated myelopathy, stiff-person syndrome, polyradiculoneuropathy). 





