Clinical information
Anti-GBM disease is a type of small vessel vasculitis. It is characterised by the presence of autoantibodies against the non-collagenous domain 1 of the α3-chain of type IV collagen (α3(IV)NC1). The target antigen is localised in the glomerular basement membrane of the kidney and in the basement membrane of the pulmonary alveoli. The majority of patients suffer from rapidly progressive glomerulonephritis with micro- or macrohaematuria, usually mild proteinuria and anuria. If the kidneys and lungs are affected (as in 60 to 80 % of patients), it is called Goodpasture's syndrome. In 20% to 40% of patients with anti-GBM disease, only the kidneys are affected, in a small proportion only the lungs. Untreated, anti-GBM disease can quickly lead to renal failure, lung failure and death. Its incidence is estimated at 0.5 to 1.6 cases per million per year. Anti-GBM autoantibodies are pathogenic:: high titers usually occur in patients with rapidly progressive kidney disease. If the antibodies are removed early by plasma exchange, the prognosis improves. Relapses are rare if anti-GBM autoantibodies are no longer produced after plasma exchange and under immunosuppression. If anti-GBM autoantibodies can be detected in the blood before a kidney transplant, a relapse in the transplanted kidney is very likely.
Diagnostics
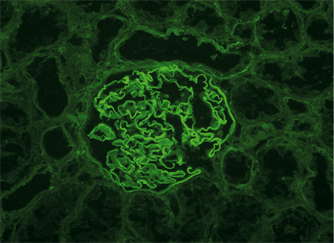 The diagnosis of anti-GBM disease in patients with symptoms of glomerulonephritis with or without lung involvement is based on the detection of anti-GBM autoantibodies in serum or kidney tissue. The antibodies can be determined in the indirect immunofluorescence test (IIFT) using frozen sections of monkey kidney or in monospecific immunoassays with purified NC1 domain (e.g. ELISA, ChLIA, line blot, antigen dots in IIFT). Detection of the antibodies in a kidney tissue sample helps to confirm the diagnosis. Up to 35% of patients with anti-GBM disease have antibodies against the cytoplasm of neutrophil granulocytes (ANCA, mostly against myeloperoxidase (MPO)). Up to 10% of patients with ANCA have anti-GBM autoantibodies. In the case of a negative serological result and a continuing suspicion of anti-GBM glomerulonephritis, a kidney biopsy is advisable.
The diagnosis of anti-GBM disease in patients with symptoms of glomerulonephritis with or without lung involvement is based on the detection of anti-GBM autoantibodies in serum or kidney tissue. The antibodies can be determined in the indirect immunofluorescence test (IIFT) using frozen sections of monkey kidney or in monospecific immunoassays with purified NC1 domain (e.g. ELISA, ChLIA, line blot, antigen dots in IIFT). Detection of the antibodies in a kidney tissue sample helps to confirm the diagnosis. Up to 35% of patients with anti-GBM disease have antibodies against the cytoplasm of neutrophil granulocytes (ANCA, mostly against myeloperoxidase (MPO)). Up to 10% of patients with ANCA have anti-GBM autoantibodies. In the case of a negative serological result and a continuing suspicion of anti-GBM glomerulonephritis, a kidney biopsy is advisable.
Files
Antibody detection in autoimmune nephropathies

























